
When the deliverable had to do the job the organization wasn't ready to do yet.
Leading provider research inside an organization mid-transformation, where twelve stakeholders across eight kickoff sessions surfaced five different versions of what we'd been hired to do, and the journey map had to function as decision-making infrastructure for an org that didn't yet have any.
- Client
- A global leader in connected health and medical devices
- Year
- 2025
- Role
- Service designer and research lead
ProcessTimeline component populated with the four phases of this engagement: (1) Stakeholder kickoff — 8 sessions, 12 stakeholders, weeks 1–2; (2) Provider research design + recruit recovery + execution — 10 interviews, in-person to remote pivot, weeks 3–8; (3) Synthesis — three iterations to design implications, weeks 8–11; (4) Opportunity workshop — two days with product, CX, research, week 12. Use src/components/ProcessTimeline.astro.
Cross-case convention: every case opens with a 'what the project included' graphic near the top, so the scope of the work is visible in the first 90 seconds before the reader commits to deeper reading. Currently the case asks the reader to infer scope from prose.
Stakeholder map of the twelve people in the eight kickoff sessions, anonymized (titles and reporting structures only, no names). Goal: a visual that lets the reader see the org shape (six geographies, two newly-restructured leadership functions, IC design teams scattered across time zones) before they read the prose.
Anchors the 'twelve stakeholders described five different engagements' claim with a visual establishing shot of the room I walked into, so the asks-paragraph below lands faster.
In the first two weeks, twelve stakeholders described five different engagements.
The engagement opened with standard kickoff interviews: eight sessions, twelve stakeholders across the client organization, ranging from a senior product leader less than eight months into his role and a newly-appointed CX leader (freshly moved from a product-aligned reporting structure to a horizontal one) through directors of adjacent functions, an internal user researcher, a project sponsor, and the IC design teams who would be the day-to-day partners on the work.
The product leader wanted a framework. Something consistent, scalable across six geographies, with shared language and governance, to coordinate decision-making across product teams that had been operating independently for years. The CX leader wanted something different: research that would shift the conversation inside the organization, give CX a credible voice in strategic prioritization, and help engineering-DNA product teams sit in the problem space before defaulting to solutions. A research leader wanted methodology. Two adjacent function leads wanted the work to land in their roadmaps. The IC design teams wanted the engagement to be useful to the work already in flight, which was a different ask again.
The contradiction was audible across the kickoff interviews themselves. By the time we’d sat with the twelfth stakeholder, no two had described the same engagement. A shared understanding of what we’d been hired to do hadn’t actually arrived yet.
The call I made was that the research had to do double duty: deliver findings and quietly build the shared understanding the engagement should have started with. That choice shaped everything I designed over the next twelve weeks.
What I led, and how I led it.
I worked as service designer and research lead on the three-person core team from kickoff. What I owned across the engagement:
- The end-to-end research approach for the provider research: study plan, recruiting strategy, and the interview protocols for both the sleep specialists and the home medical equipment respiratory therapists
- The screener and recruiting brief
- Moderation of the majority of the ten 90-minute provider interviews
- The operating infrastructure of the research itself: interview tracker, calendar coordination, session role assignments, the templates the team filled in during interviews
- A client onboarding video. Our clients participated as observers in the research sessions, and I built a video that taught them where to take notes, how to use the templates I’d built, and where to save what, so the sessions started from a shared baseline instead of a setup conversation
- Facilitation of the majority of the sessions and debriefs
- Three iterations of the synthesis, including the two that didn’t land
- The design implications work that became the foundation for the opportunity workshop
- Recruiting recovery when our recruiting partner fell behind
The engagement lead held the strategic frame and stakeholder relationships, and pushed me hard on the synthesis until it landed. A senior service designer co-owned the visual journey artifact. The opportunity workshop was designed collaboratively across the team. An intern joined partway through. The team operated across three time zones: North America, Europe, and Australia.

Designing the provider research
Ten 90-minute remote interviews in June and July: three home medical equipment respiratory therapists and seven board-certified sleep-specialist physicians. I moderated the majority. Each interview walked the participant through a consistent enough structure to enable cross-interview synthesis, open-ended enough to let the participant lead me into territory I hadn’t anticipated.
The dual-brief problem from synthesis shaped how I wrote the discussion guides, specifically the depth of the questions and what they were optimized to surface. The product leader’s framework question needed the interviews to surface patterns the team could organize around. The CX leader’s culture-change question needed them to produce moments that could shift a room. So the protocols were built to do both: a structural arc of “walk me through a typical patient from referral to ongoing care” that produced comparable cross-interview data, with embedded prompts (“tell me about the last patient who surprised you,” “what’s the moment in this week you keep thinking about”) that produced the specific scenes I’d need later. The social-meter line and the paint-by-numbers metaphor both came from those scene-prompts, not from the structural arc.
When the original plan died
The original study was designed in-person. The client had told us at kickoff they could handle recruiting from their own database, with an internal person assigned to run it. We built the study around that promise: tighter geographic scope, larger sample, in-person sessions that let the team observe how providers worked in their real environments.
Two things happened. The internal recruiter got pulled to other work without warning. And the recruiting capability the client had presented to us turned out to be more aspirational than real; what was actually available was sending a survey to an internal list. By the time that surfaced, we had almost no time to recover.
We had raised the flag earlier about the client’s pre-approved external recruiting firm, which had disappointed my team lead on a prior engagement. The client pushed back: this time would be different. With the internal capability collapsing and the timeline gone, we had no other option, so we routed to the firm.
The only way to find enough participants in the time we had left was to widen the geographic net, which meant switching from in-person to remote. I rewrote both provider protocols for remote delivery and reset the operational scaffolding around remote sessions: observer onboarding, note-taking templates, time-zone-friendly scheduling. The team executed against the new plan in a compressed window.
Even with the pivot, we ended with a smaller sample than the study had been designed to support: three home medical equipment respiratory therapists and seven sleep-specialist physicians. The final deliverable carries an explicit recommendation that further research validate and deepen the HME archetype.
What the research found
The two provider archetypes are living in two different versions of the same broken system, and the patient is sitting in the gap between them.
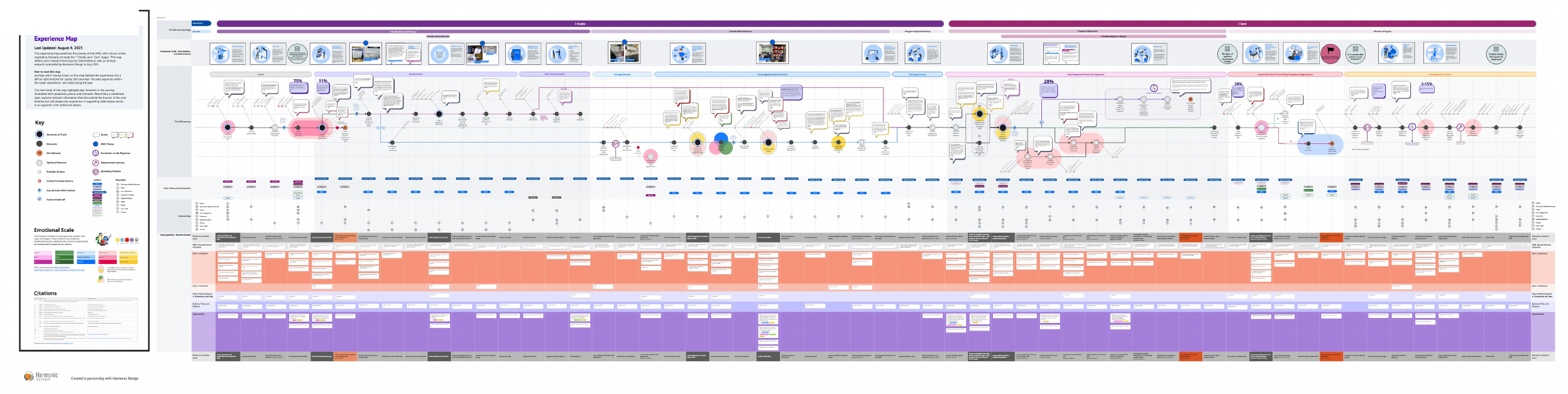
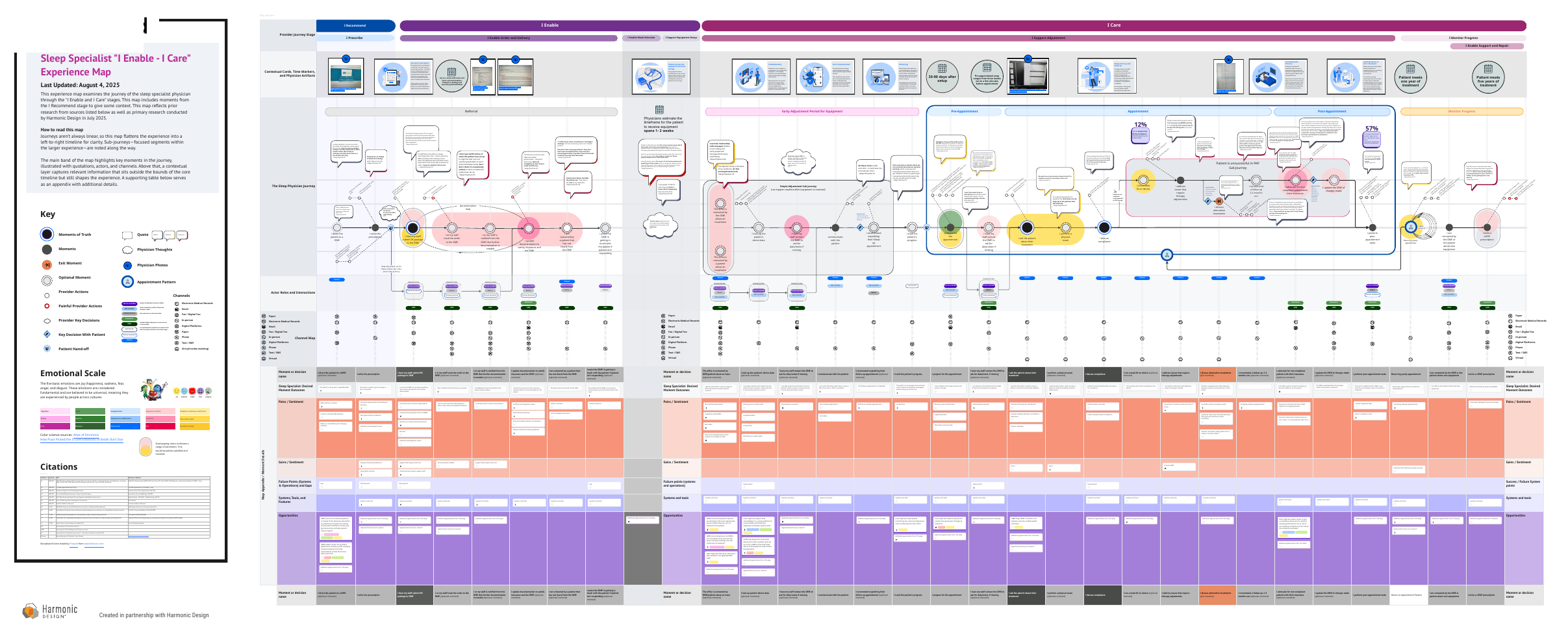
The maps used the same visual vocabulary so the team could read them together: same emotional curve, same channel rows, same set of detail tables underneath. That parallelism is the move that exposed the structural finding below.
Sub-journey maps that sit underneath the two big archetype maps. Whitney to send: which sub-journeys, what they show, and whether they belong as a grid of thumbnails or as a single composite. Likely candidates: prescription, initial setup / fitting, ongoing adherence, troubleshooting, insurance/compliance handoff.
The two big maps carry the structural-gap finding, but the sub-journeys are where the operational detail lives. Hiring managers reading at craft depth will want to see that the team mapped not just the overall arc but the moments inside it.
The respiratory therapist: a dedicated guide shouldering emotional weight
Respiratory therapists derive genuine meaning from helping patients overcome fear and start therapy, and work at for-profit companies whose patients regularly accuse them of putting profit before care. The setup model is collapsing under them: full-service in-person appointments are being phased out and replaced by drop-shipped equipment and the therapist functioning as remote tech support. One participant told us the most frustrating part of her job was that she could no longer put her hands on the equipment a patient was struggling with.
After a long week of convincing people that it will be okay, your social meter is just a little gone.
The sleep specialist: an artist forced to paint by numbers
Physicians described being boxed in by four pressures at once. Time: one told us his practice was being asked to see five to six hundred new patients a week and was “literally not able to take care of them all.” Insurance: the four-hour-a-night, twenty-one-day compliance rule shaped clinical decisions whether or not the physician thought it was clinically right. Technology: an EMR that didn’t integrate with the equipment provider, a separate compliance reporting platform, and a patient messaging tool one physician called “free uncompensated work.” Management: decisions made above them about which equipment providers they could refer to. They wanted to provide individualized care; the system was optimizing for throughput and reimbursement.
Redrawn 'Physicians Are Boxed In' four-quadrant diagram. The existing version from the insights deck is too rough for the case study. Needs to be remade clean: physician at center, four constraint quadrants (Time, Technology, Insurance, Management), each labeled with a one-line specific (e.g. Insurance: 'four-hour-a-night, twenty-one-day compliance rule').
This is the visual that makes the 'artist forced to paint by numbers' framing legible at a glance. Without a clean version, the section relies entirely on prose and the visual undersells the structural read.
The patient sits in the gap
The structural finding that mattered most for the client’s strategy emerged from comparing the two archetypes. One sleep specialist named it cleanly: when the equipment provider fails the patient, the patient does not blame the equipment provider. The patient blames the physician who sent them there.
They look at the equipment provider as my extension. I’m the one who sent them there.
The prescribing physician owns the relationship and bears the reputational risk. The equipment provider runs the day-to-day experience. The patient sees one continuous service. No actor in the system has authority over the whole thing. This is the structural gap a connected-health platform is positioned to occupy, and it became the through-line of the workshop two months later.
Synthesis as craft
The synthesis was the part of this engagement where I learned the most, and where my work failed before it succeeded.
My first version of the insights deck organized the findings around the structure of the interviews: what we heard from respiratory therapists, what we heard from physicians, what cross-cut both. It was comprehensive. It was also unusable. It gave the team everything we had heard without giving them a way to act on any of it.
My engagement lead pushed back. The second version tried to fix the structural problem by adding a layer of synthesis on top of the interview findings. It was better. It still was not right. The synthesis layer was descriptive rather than directional. It told the team what was true. It did not tell them where to look.
The third version reorganized everything around design implications. For the respiratory therapists: human touch (operations were optimizing for cost, but referrals depended on human-quality experiences) and patient misconceptions (RTs were exhausted from working against age-old patient anxieties about therapy). For the physicians: boxed in (clinical autonomy under siege from outside forces), time pressure (rising patient volumes, messaging tools as unpaid labor), information up front (delays caused by missing context that better data could surface), and trust in equipment providers (physicians needed confidence in who they were referring to). Each implication paired evidence from the interviews with a directional question: how can the company use its position to do something about this?
The third version was shorter than the first and did less. It was the version that worked.
The first version was a research summary. The third version was a design brief. I had been treating those as the same thing. They are not.
The lesson I took: synthesis is a craft separate from research. The version that captures everything you heard is rarely the version that gives the team something to act on. An engagement lead pushing back is the work functioning correctly. I am planning for that revision cycle on subsequent projects rather than treating it as a setback.
The opportunity workshop: where the artifact became infrastructure
The workshop was the moment the artifact stopped being a research deliverable and started being decision-making infrastructure.
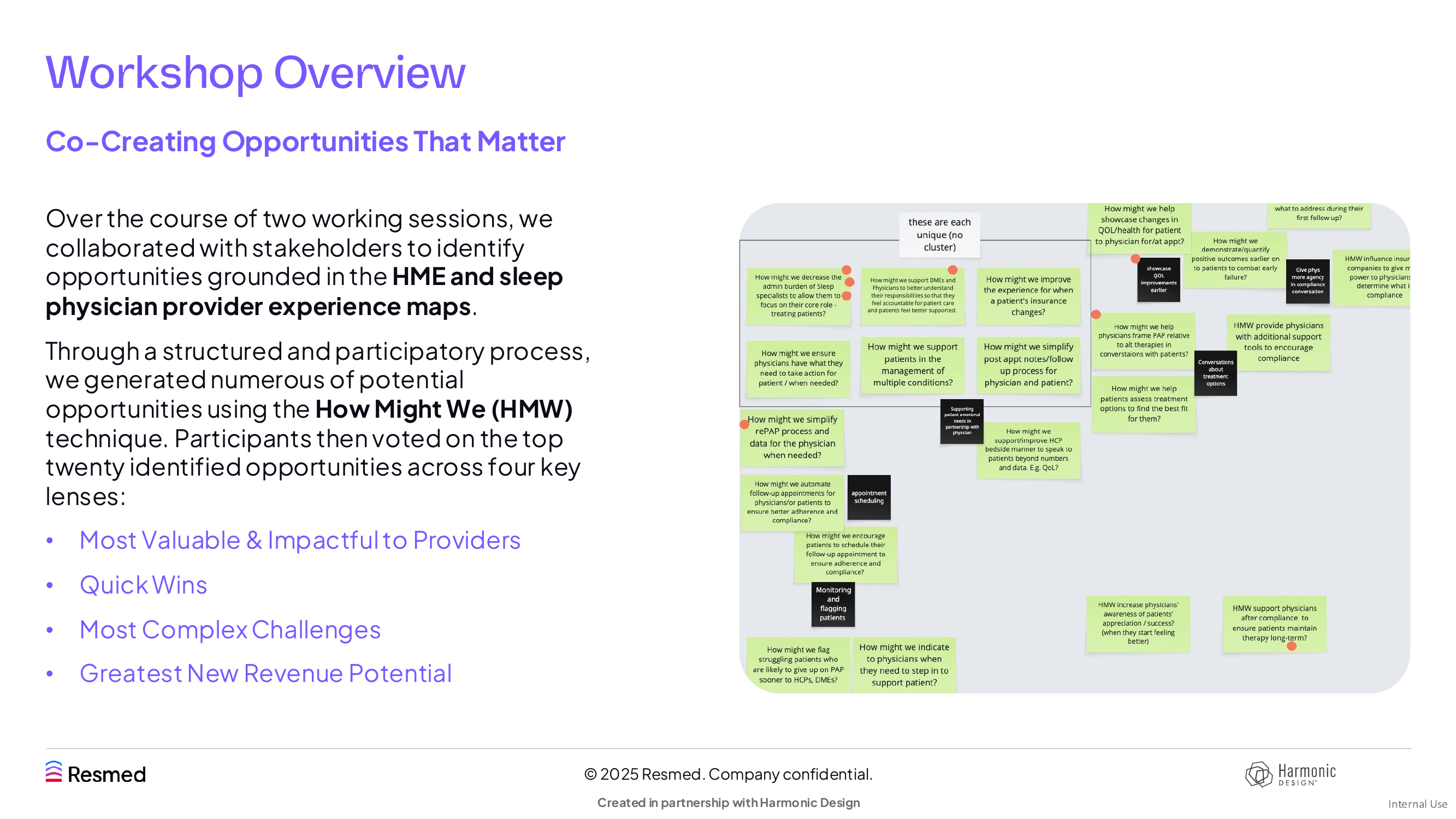
We ran two sessions at the end of July with the client’s product, CX, and research teams. Day one opened with a research presentation walking the team through the maps and the design implications, then moved into structured “How Might We” generation grounded in specific moments on the journey. Day two was synthesis and prioritization: participants voted across four lenses (most valuable to providers, quick wins, most complex challenges, greatest revenue potential) on the twenty most promising opportunities.
Five themes surfaced from the prioritized opportunities: patient communication (moving away from phone-based outreach), mask fit and selection (a moment of truth that drove cost and adherence), coordination and data consolidation (the broken handoff between physician and equipment provider), compliance and monitoring (the four-hour-a-night problem), and insurance and policy management (the prior-authorization burden).
The workshop did the job the CX leader had asked for in the stakeholder interview, before any provider research had been conducted. She had wanted Product and CX in a room arguing about customer problems together. The maps became the thing the room argued about. That outcome was not accidental. It was the function we’d been designing toward since week one. We built into the workshop a discussion segment on rituals and governance, explicitly framing how the maps could continue to live and evolve after the engagement ended. Both leaders walked out of the second day with what they had asked for, in different forms.
What the work was set up to do next
The engagement closed at the end of August with the maps, the design implications, and the prioritized opportunities handed off to the client’s product and CX teams. The maps were designed to keep working after we left. Each map carries the same structural vocabulary, so a product team in any of the six geographies can read either archetype against their own roadmap and locate themselves on it. The prioritized themes from day two were scoped to be picked up as discovery streams rather than as a single mega-program, which is what the product leader had asked for in week one.
I do not yet know which of the five themes the client has moved on, and the NDA prevents naming specifics even where I do know. What I can say is that the test of this work is not whether the workshop happened. It is whether the maps continue to function as the shared object the room argues over six and twelve months from now, and whether the rituals we sketched on day two get built. Those are the questions I’m tracking on the next engagement with this client.
Three things that traveled with me out of this engagement.
Reading the business is design work. The most important insight from this project did not come from the provider interviews. It came from holding five different versions of the engagement at once, inside an organization mid-transformation, and deciding what the research had to do about that. That read came from a decade operating in international development, nonprofits, and digital strategy before I came to service design, and from an MBA spent learning how organizations actually make decisions. Stakeholder navigation is not a soft skill adjacent to the design problem. For me, it is the design problem, and it is where the cross-domain pattern-matching I built before this career compounds.
Synthesis is iterated, not produced. I drafted two versions of the insights deck before I drafted the one that landed. The lesson was not that I should have been more careful upfront. The lesson was that the first version is rarely the one that earns its place, and that an engagement lead pushing back is the work functioning correctly. I plan for that revision cycle now.
Group sessions surface intent; one-to-ones surface the gaps. The original plan died because the internal recruiter’s actual capability did not match what kickoff had described. We had raised the flag about the external firm and been overruled. The miss that mattered was earlier and quieter: I treated group sessions and written briefs as enough to assess the internal recruiter’s capability, when only an hour with him alone, walking step by step through how he would actually run the recruit, would have surfaced the gaps. That hour is the move I’m running on the next engagement before any methodology is built around an operational dependency.